

Abstract
OBJECTIVES
Nilotinib is a potent, second generation inhibitor of BCR-ABL tyrosine kinase (TKI) and represent a standard of care for patients with chronic myeloid leukemia (CML), including accelerated phase (AP-CML). In 2005, we initiated a phase 2 study of nilotinib 400 mg twice daily as a frontline therapy in patients with AP-CML, and herein present the efficacy and safety data after a median follow-up of 68.4 months (range, 0.3-124.8).
METHODS
This was a prospective, single institution, phase 2 study in patients of age ≥18 years with a newly diagnosed, untreated AP-CML (except for <1 month of previous imatinib) defined according to MD Anderson criteria (Kantarjian, 1988). Patients were treated with nilotinib 400 mg twice daily (BID). Data are presented on an intention to treat analysis with a cutoff date of June 30st, 2018.
Response criteria are standard. Fisher exact test and χ2 were used for analysis of categorical variables; and survival probabilities were estimated using the Kaplan-Meier method. Time to events (e.g., overall survival, event free survival) was calculated from the date of treatment to the date of an event or to last follow-up as previously reported (Cortes et al, 2010).
RESULTS
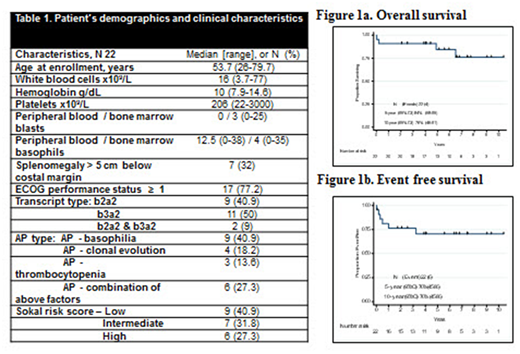
Twenty two patients of a median age of 53.7 years (range, 26-79.7) were enrolled. Table 1 summarizes clinical characteristics of all patients. The median treatment duration was 47.3 months (range; 0.3-124.4), and the median follow-up 68.4 months (range, 0.3-124.8). All patients discontinued study as of January 2017 due to planned study closure; but 11 patients (50%) continued on nilotinib off protocol at data cut-off (400 mg BID [3]; 300 mg BID [2]; and 200 mg BID [6]). Median time to treatment discontinuation in the remaining 11 patients was 12.9 months (range, 0.3-112); reason for discontinuation was: inadequate response [3], toxicity [2], non-compliance/financial [4]; elective discontinuation after sustained MR4.5 >2 years [1]; and death due to stroke [1].
Sixteen patients (73%) achieved complete hematologic response (CHR). Overall rates of CCyR, MMR, MR4.5 and CMR (undetectable transcripts with at least 100,000 ABL copies) were 73%, 73%, 55%, and 41%, respectively. Median times to CCyR, MMR, and MR4.5 were 2.9 months (range, 2.7-6.4), 5.7 months (range, 2.7-99.2) and 6.0 months (range, 2.7-36), respectively. Seven patients (32%) achieved sustained MR4.5 >2 years.
In total, 4 patients lost their best achieved response (CHR [1], CCyR [2] and MR4.5 [1]) while on study. All events were associated with acquired ABL domain mutation; Y253H [2], T315I [1], and F359I [1] with a median time to detection of 16.7 months (range, 7-40).
During the study conduct, one patient progressed to blast phase after 2 months on nilotinib. Two patients died while on study, one due to stroke and one due to unrelated medical condition, after being on therapy for 3 and 0.4 months, respectively.
One patient electively discontinued nilotinib after being in sustained MR4.5 for 107 months, and remains in MR4.5 after 6 months off therapy. Estimated overall survival and event free survival at 5 years were 84% and 70%, respectively (Figures 1a & 1b).
On univariate analysis, age >55 years was associated with lower rate of MMR (p = 0.034; HR 0.34; 95% CI 0.12-0.92); MR4 (p = 0.013; HR 0.25; 95% CI 0.08-0.75); and MR4.5 (p = 0.01; HR 0.15; 95% CI 0.04-0.63). Overall survival was inferior in patients older than 55 years (p = 0.014; HR 2.4; 95% CI 2.36-not estimated); and in those with > 1 AP-CML defining abnormality (p = 0.018; HR 9.53; 95% CI 0.98-92).
The most frequent non-hematologic adverse events (AEs) were hyperbilirubinemia (63% of patients), rash (63%), hypertension (59%), and transaminitis (50%). Grade ≥3 AEs observed in more than one patient were hyperbilirubinemia (n=2), and transaminitis (=2). Two patients developed arterio-thrombotic AEs: stroke and myocardial infarction (one each).
Hematologic AEs included (all grades; grade ≥3): anemia (36%; 9%), thrombocytopenia (32%; 14%) and neutropenia (14%; 9%). Two patients (9%) discontinued therapy due to nilotinib related AE, one for G3 peripheral neuropathy and one for G3 hyperbilirubinemia with G2 thrombocytopenia.
CONCLUSION
Nilotinib is safe and highly effective in patients with AP-CML, and induces fast and durable responses. More than 50% of patients can achieve MR4.5. Clinical trial.gov: NCT00129740.
Cortes:novartis: Research Funding. O'Brien:Pfizer: Consultancy, Research Funding; Janssen: Consultancy; Aptose Biosciences Inc.: Consultancy; Kite Pharma: Research Funding; Regeneron: Research Funding; Vaniam Group LLC: Consultancy; Amgen: Consultancy; Pharmacyclics: Consultancy, Research Funding; Celgene: Consultancy; Alexion: Consultancy; Abbvie: Consultancy; GlaxoSmithKline: Consultancy; Acerta: Research Funding; Gilead: Consultancy, Research Funding; Sunesis: Consultancy, Research Funding; Astellas: Consultancy; TG Therapeutics: Consultancy, Research Funding. Konopleva:Stemline Therapeutics: Research Funding; Immunogen: Research Funding; abbvie: Research Funding; cellectis: Research Funding. Verstovsek:Incyte: Consultancy; Celgene: Membership on an entity's Board of Directors or advisory committees; Italfarmaco: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau. Kadia:Celgene: Research Funding; Jazz: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Novartis: Consultancy; Abbvie: Consultancy; BMS: Research Funding; Novartis: Consultancy; Takeda: Consultancy; Celgene: Research Funding; BMS: Research Funding; Pfizer: Consultancy, Research Funding; Amgen: Consultancy, Research Funding; Jazz: Consultancy, Research Funding; Abbvie: Consultancy; Takeda: Consultancy; Amgen: Consultancy, Research Funding. Ravandi:Macrogenix: Honoraria, Research Funding; Orsenix: Honoraria; Orsenix: Honoraria; Astellas Pharmaceuticals: Consultancy, Honoraria; Xencor: Research Funding; Sunesis: Honoraria; Bristol-Myers Squibb: Research Funding; Astellas Pharmaceuticals: Consultancy, Honoraria; Jazz: Honoraria; Abbvie: Research Funding; Bristol-Myers Squibb: Research Funding; Seattle Genetics: Research Funding; Macrogenix: Honoraria, Research Funding; Abbvie: Research Funding; Amgen: Honoraria, Research Funding, Speakers Bureau; Amgen: Honoraria, Research Funding, Speakers Bureau; Jazz: Honoraria; Sunesis: Honoraria; Xencor: Research Funding; Seattle Genetics: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal